




Until recently, preborn lives in Northern Ireland (NI) were significantly more protected than they are in the United States. But that changed legally in October 2019. Both Lives Matter—an organization that seeks “to re-frame the abortion debate in Northern Ireland and beyond, advocate for better care in pregnancy crisis, and create a culture that values every woman and her unborn child”—was ready to stand for life, continuing the work they’ve been doing since 2017.1https://bothlivesmatter.org/
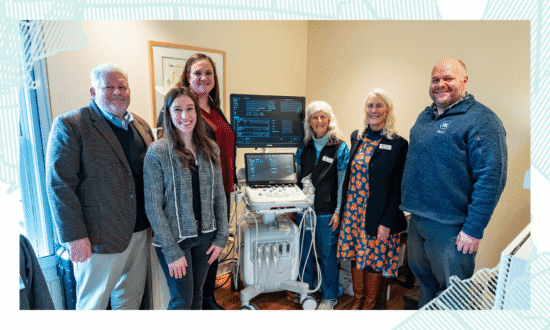
Dawn McAvoy, co-founder, and Marion Woods, services advocate, work tirelessly to change the way life is viewed and received in their culture. In the summer of 2021, several representatives from the ERLC, including myself, visited Northern Ireland and delivered an ultrasound through the Psalm 139 Project to Both Lives Matter. While there, McAvoy and Woods answered some questions about the state of abortion in NI and how the church in the U.S. can help them care for the vulnerable in their midst.
Elizabeth Graham: Can you give me a brief history of abortion in Northern Ireland and where things stand today?
Dawn McAvoy: Up until Oct. 22, 2019, abortion was legal in NI, but it was, in the famous phrase, “safe, legal and rare.” It was legal, but it was very rare because the law put a very high bar on who could access abortion within the health service here. In legal terms, a woman could terminate a pregnancy if her life was at risk, which is very rare, but also if her mental health was at risk, defined by law to be in a way that was real, serious, long term, or permanent. The bar was set so high that abortions here were very restricted.
There was a certain amount of harsh language [in the law], but there was also compassion. We would have said that the law recognized and protected both lives, with abortion being very rare. On an annual basis, and compared to the rest of the United Kingdom, abortion rates in Northern Ireland were seven times lower. In the rest of the United Kingdom—England, Scotland, and Wales—abortion law had changed in 1967 in a way that effectively opened the door to abortion on demand.
We had a restrictive abortion law for 50 years. When our campaign launched in 2017, we did some research to see if the law makes a difference. We knew our law was restrictive. We knew abortion rates were lower. We knew some women went to the rest of the United Kingdom to access abortion. But what did that mean? Rather than thinking of it in terms of “lives ended,” we wanted to show that lives were being lived in Northern Ireland that otherwise wouldn’t have been.
We looked at abortion rates over those 50 years, and we were able to say with confidence that a conservative and plausible estimate was that 100,000 people were alive in Northern Ireland who would not have been if the law had been changed here in 1967.
We shared this on billboards, and that campaign was challenged. It was reported to the Advertising Standards Authority in England. They investigated our research, upheld our claim, and rejected the complaints against us. So, we knew that the law here had made a difference. It recognized and protected both lives, and lives had been saved.
In 2019, all of that changed when Westminster (the U.K.’s seat of government) intervened in a devolved government in Northern Ireland [a situation caused when one political party refused to participate in the role of government, which then allows Westminster to dictate laws and procedures].2https://erlc.com/resource-library/articles/explainer-whats-happening-in-northern-ireland/ Westminster introduced an amendment to a funding bill related to NI’s government that decriminalized abortion [as well as permitted same-sex marriage]. This removed the law that we were operating under. For six months, we were in a position where there was no law on and no regulatory framework for abortion.
At the end of March 2020, the new regulations were published. We went from being one of the jurisdictions in Europe that was the most restrictive on abortion and was the most protective for both lives, to a place where we’re now one of the most liberal or permissive abortion regimes on paper. There is no criminal sanction for a woman who wants to terminate her own pregnancy right up to birth. Within the regulatory framework, there is no restriction on abortion up to 12 weeks. There’s no need to provide a reason for a termination. You can access abortion on request and on an undefined, undiagnosed mental health basis up to 24 weeks. It’s being framed around the same legislation that operates in England, Scotland, and Wales.
What this means practically is that a woman just needs to be able to say, “My circumstances aren’t appropriate”—whether that’s a lack of finances, lack of emotional support, career pressures—and there will be no questions asked. If there’s somebody that will provide the abortion, you can have the abortion. You can receive an abortion up to birth in cases of a diagnosis of fetal abnormality, disability, or a terminal illness.
On top of that, we have limited conscience protections for doctors, nurses, and healthcare professionals who would object to being involved in an abortion. So, administratively, there are lots of questions as to who can withdraw from the procedure, especially now because it’s not just surgical, but chemical abortions.
A really concerning aspect of the new law has been how it addresses education, so that within the school system, how abortion is taught regarding the sanctity of human life or human dignity has all been impacted by what Westminster did in 2019. Abortion services haven’t been centrally commissioned yet from the Department of Health; it’s not on paper. But time will tell how it’s implemented in reality.
EG: For our audience’s sake, help us understand the implications to the national health system, as well as the implications to the third-party abortion providers. What are the differences between what we face in the U.S. versus what you all are facing in Northern Ireland?
DM: In the United Kingdom, we have a system called the National Health Service, which is medical care that’s free, at the point of need, for everyone. Some people will choose to go privately, but you don’t have to. From childhood right up until death, we all have free healthcare.
When it comes to abortion, it is under the NHS. But the NHS does not carry out abortions. Only 1% of abortions are performed within National Health Service hospitals or clinics. Ninety-nine percent of abortions are outsourced to private providers. The vast majority are private providers who are paid for by taxes. You have Planned Parenthood in America. In the United Kingdom, we have the British Pregnancy Advisory Service. BPAS and Marie Stopes would be the two largest abortion providers.
EG: In the U.S., the conversation usually groups abortion as a part of women’s reproductive healthcare options. In the United Kingdom, they’ve disconnected the abortion service from the national health care system. So, is it correct that the woman who might seek a termination is not actually receiving any type of continuum of care unless there is a problem that arises from the third party who administers the abortion, whether it’s physical or chemical?
DM: Technically it all comes within the NHS, but you’re absolutely correct. A woman could go to her general practitioner (GP), discuss her options, and could be pointed from there to the abortion provider. But she doesn’t have to do that. She could directly phone the abortion provider. This is one of our concerns. In the U.K. system, we all have a healthcare number. There’s good data collection on our medical records, but for the purposes of abortion, your medical records can be disconnected.
We know that abortions can be accessed under a false name, address, and doctor’s practice. If a woman has an abortion, her medical records through their GP’s practice may not align. So, it can be difficult to prove the negative long-term impact of abortion on physical or mental health unless someone comes forward and says, “I had an abortion, and these are the side effects.”
There is also the concern that the potential side effects are not being explained, especially with the rise of telehealth medicine and the chemical abortion pill. For example, if a woman experiences side effects, she would go back to the abortion provider in most cases. She may phone them and say, “I think I’m bleeding more heavily than I expected, or I have some more painful cramps than I expected.” But if the bleeding or cramps are outside a particular standard, she would go to the emergency department at the local hospital. This means that the information wouldn’t be linked to the abortion provider. If there’s a serious side effect—and as many as 1 in 20 women experience significant side effects—it is generally dealt with back within the NHS and not necessarily connected to the abortion.
EG: And NHS is paying the abortion clinic for those services, but abortion clinics are not responsible for caring for her after her termination?
DM: No, not if it’s what would be deemed to be a severe or serious side effect.
EG: How is Both Lives Matter working to influence the culture in Northern Ireland to value the dignity of every human life?
DM: When we launched in 2017, our vision statement was that we imagine a people in place who value the life and health of women and unborn children and pursue the well-being of both. We always talk about both lives, mommy and baby. So, we wanted to immediately challenge the perceptions that we don’t care about the woman. For us, there is a beautifully unique biological and relational aspect to a pregnancy. You can’t talk about one life without the other. It’s always both lives, pre and post-birth.
It’s also not just about saying no to abortion. The law said no to abortion in the vast majority of cases for 50 years. We could safely say that the 98% of abortions that happen in Great Britain for socioeconomic circumstances weren’t happening in Northern Ireland. And less than the other 2% were, as well. It was good that the law said no to abortion, but that doesn’t necessarily help a woman when she’s facing a pregnancy crisis.
We want a trinity of provisions for both lives: laws that protect all life from fertilization to natural death; services that enable every life and enable women to choose life; and a culture that affirms all of life, regardless of the circumstances of conception and the sex, age, health, ability, or disability of the baby.
The other thing we wanted to do was challenge that it’s a religious argument. Both Lives Matter isn’t a religious campaign. We are open to people of all faiths and no faith. Yes, the values that we operate on are faith-based. Within the context of a church conversation, we will talk about Scripture and a biblical argument for human dignity and being made in the image of God.
But when in the public square, talking to the media, and talking to community groups, we don’t believe that you need to have our same beliefs. Science says when life begins. Medical science and lived experience tells us what every pregnancy means and can result in when it goes to its natural conclusion. So talking about those lived experiences, medical science, the difference the law makes, and the cultural agenda, we think we can reframe the abortion conversation to take it outside of the religious box and the anti-woman box it is put in, and talk about both lives.
It’s a much more beautiful story for society than abortion, which results in the death of one life and very often harms the remaining life of the woman.
EG: We want to make abortion unnecessary and unthinkable while also working to restrict laws, because as we work to restrict laws, more lives are saved. But it doesn’t change hearts, minds, behaviors, and actions. So we firmly believe that to make abortion unthinkable, an education has to happen while also serving women to make abortion unnecessary. How can Christians and churches in the U.S. support the work that you all and other organizations are doing in Northern Ireland?
DM: I don’t think there is a disconnect between the church in America and the church here. You’ve experienced a culture of abortion for nearly 50 years. You know what it has done to society. You know how it reshapes and changes how lives are considered and viewed, preborn and post-birth life. You know the impact that it has had on women because you’ve seen the rates of abortion. There’s a lot that you’ve experienced that we haven’t yet, so you can pray for us.
As the church in America addresses the subject of abortion—within the church and then from the church into society—that will impact what the abortion culture is like here. The impact of what America does with abortion actually ripples across to the U.K.
Marion Woods: I like the collaboration in the church in America. That sets a very important example for the churches here. It is one of our hopes and dreams for Both Lives Matter that our churches collaborate on this issue. And the more that we work together on this issue, the more it shines a light on the fact that ultimately, as people who are following Jesus and rooted in the Bible, human dignity comes to the forefront.
Being made in the image and likeness of God reminds us that, regardless of denominations, we are all protecting the gift of life that God has blessed us with. We remind people in churches that Jesus himself spent time as an embryo. Regardless of the church background we might come from, we can unify around the truth that life is a gift given to us because God is our Creator, and we are his creation.
EG: Is there any encouraging information or story of hope that you could just share with us today as we’re wrapping up our time together?
DM: We haven’t had an abortion culture. We haven’t had abortion clinics, so we haven’t had the need for pregnancy resource centers as you would know them in the states. But, it’s always been our heart as an organization. The gift of the sonogram machine [through the Psalm 139 Project] and seeking to love us—the church and mommies and babies—in the name of Jesus and bring glory to God has been such an encouragement during a time of darkness and a season of lament, grieving, and pain. I think we’re still trying to come to terms with and understand it.
The gift of this sonogram machine will expose the lie that there is no life [inside the womb]. It will reveal the truth of new life. That has been one of the most hopeful, encouraging, and tangible expressions of a community of a collaboration—all in the name of both lives—that we have that we have felt in the past year and a half, which has been so dark. So, thank you.
Dawn McAvoy is co-founder of Both Lives Matter.
Marion Woods is services advocate for Both Lives Matter.