
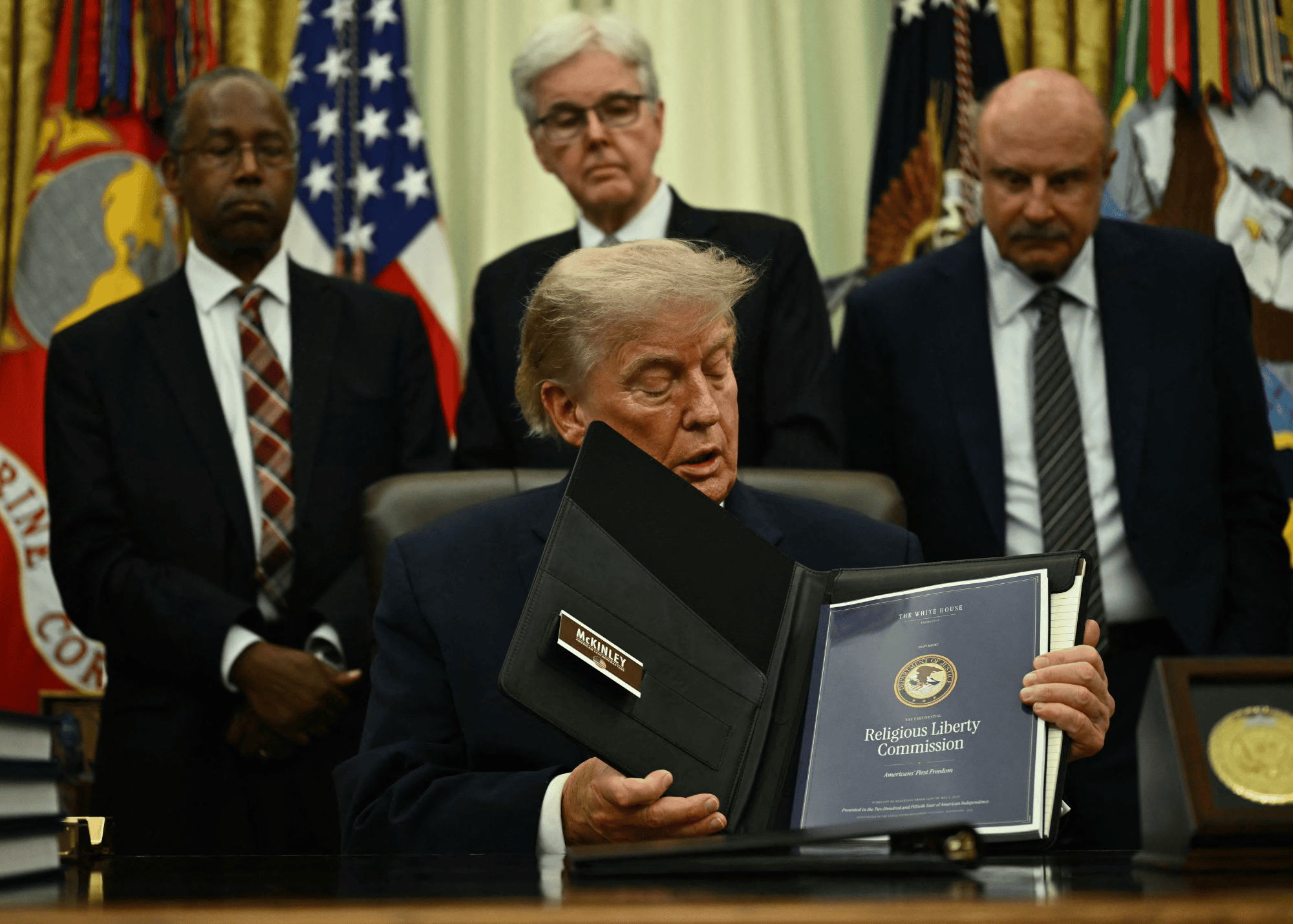



“Few topics are as complex and controversial as human sexual orientation and gender identity,” says Lawrence S. Mayer and Paul R. McHugh. “These matters touch upon our most intimate thoughts and feelings, and help to define us as both individuals and social beings. Discussions of the ethical questions raised by sexual orientation and gender identity can become heated and personal, and the associated policy issues sometimes provoke intense controversies.”
In an attempt to shed light on these often heated discussion, Mayer and McHugh have produced a massive new 143-page report, published in the last edition of The New Atlantis, which “offers a careful summary and an up-to-date explanation of many of the most rigorous findings produced by the biological, psychological, and social sciences related to sexual orientation and gender identity.”
McHugh, the former chief of psychiatry at Johns Hopkins Hospital and arguably one of the leading psychiatrists in the world, and Mayer, a biostatistician and epidemiologist, reviewed more than 500 studies for their report.
While the report is worth reading in its entirety, it’s length may make is inaccessible to the general public. To encourage further examination of the document, I’ve compiled a list of highlights that will provide a broad and extensive—though nowhere near comprehensive—summary overview of their findings.
Sexual Orientation
Problem of Definition
• The concept of sexual orientation is highly ambiguous, and can refer to a set of behaviors, to feelings of attraction, or to a sense of identity.
• One of the central difficulties in examining and researching sexual orientation is that the underlying concepts of “sexual desire,” “sexual attraction,” and “sexual arousal” can be ambiguous, and it is even less clear what it means that a person identifies as having a sexual orientation grounded in some pattern of desires, attractions, or states of arousal.
• There are currently no agreed-upon definitions of “sexual orientation,” “homosexuality,” or “heterosexuality” for purposes of empirical research. Because of this, the authors note, “We will continue to employ ambiguous terms like ‘sexual orientation’ where they are used by the authors we discuss, but we will try to be attentive to the context of their use and the ambiguities attaching to them.”
• Longitudinal studies of adolescents suggest that sexual orientation may be quite fluid over the life course for some people and that those who report same-sex attraction no longer do so as adults.
Genetic and Innate Factors
• Research suggests that while genetic or innate factors (e.g., genes, hormones) may influence the emergence of same-sex attractions, these biological factors cannot provide a complete explanation, and environmental and experiential factors may also play an important role.
• There is some evidence from the twin studies that certain genetic profiles probably increase the likelihood the person later identifies as homosexual or engages in same-sex sexual behavior.
• The largest attempt to identify genetic variants associated with homosexuality, a study of over 23,000 individuals, found no linkages reaching genome-wide significance for same-sex sexual identity for males or females.
• The weight of evidence to date strongly suggests that the contribution of genetic factors is modest.
• Hormonal conditions that contribute to disorders of sex development may contribute to the development of non-heterosexual orientations in some individuals, but this does not demonstrate that such factors explain the development of sexual attractions, desires, and behaviors in the majority of cases.
• Studies of the brains of homosexuals and heterosexuals have found some differences, but have not demonstrated that these differences are inborn rather than the result of environmental factors that influenced both psychological and neurobiological traits.
• There is virtually no evidence that anyone, homosexual or heterosexual, is “born that way” if that means their sexual orientation was genetically determined.
Sexual Abuse Victimization and Other Environmental Factors
• One study found that bisexuals had significantly higher proportions than heterosexuals of all adverse childhood experience factors, and that homosexuals had significantly higher proportions than heterosexuals of all these measures except parental separation or divorce. Overall, homosexuals had nearly 1.7 times, and bisexuals 1.6 times, the heterosexual rate of adverse childhood experiences.
• Another study of nearly 35,000 adults found that among those reporting exposure to traumatic events, homosexuals as well as bisexuals had about twice the lifetime risk of Post Traumatic Stress Disorder (PTSD) compared to the heterosexual reference group. Homosexuals, bisexuals, and heterosexuals with same-sex partners reported experiencing worse traumas during childhood and adolescence than the reference group.
• While one study suggests that sexual abuse may sometimes be a causal contributor to having a non-heterosexual orientation, more research is needed to elucidate the biological or psychological mechanisms. Without such research, the idea that sexual abuse may be a causal factor in sexual orientation remains speculative.
• One environmental factor that appears to be correlated with non-heterosexuality is childhood sexual abuse victimization. Non-heterosexuals are about two to three times as likely to have experienced childhood sexual abuse than heterosexuals.
• In one major survey only 1.2 percent of males who had spent their adolescence in a rural environment responded that they had had a male sexual partner in the year of the survey while those who had spent adolescence living in metropolitan areas were close to four times (4.4 percent) more likely to report that they had had such an encounter.
• In that same survey women who attended college were nine times more likely to identify as lesbians than women who did not.
Distribution of Sexual Desires and Changes Over Time
• There is now considerable scientific evidence that sexual desires, attractions, behaviors, and even identities can, and sometimes do, change over time.
• While ambiguities in defining and characterizing sexual desire and orientation make changes in sexual desire difficult to study, data from these large, population-based national studies of randomly sampled individuals do suggest that all three dimensions of sexuality — affect, behavior, and identity — may change over time for some people.
• Several researchers have suggested that sexual orientation and attractions may be especially plastic for women.
• One survey found that 35 percent of self-identified gay men reported experiencing opposite-sex attractions in the past year, and 10 percent of self-identified gay men reported opposite-sex sexual behavior during the same period. Additionally, nearly as many men transitioned at some time in their life from gay to bisexual, queer, or unlabeled identity as did men from bisexual to gay identity.
Mental Health
• Compared to the general population, non-heterosexual and transgender subpopulations have higher rates of mental health problems such as anxiety, depression, and suicide, as well as behavioral and social problems such as substance abuse and intimate partner violence.
• The limited available research strongly suggests that transgender people have increased risks of poor mental health outcomes. It appears that the rates of co-occurring substance use disorders, anxiety disorders, depression, and suicide tend to be higher for transgender people than for homosexual and bisexual individuals.
• One report found that homosexual youth and adults — and women in particular — appear to be likelier than heterosexuals to smoke, use or abuse alcohol, and abuse other drugs.
• Compared to heterosexuals, members of the non-heterosexual population are estimated to have 1.5 times higher risk of experiencing anxiety disorders, 1.5 times the risk of substance abuse and about 2 times the risk of depression.
• Combined worldwide studies showed up to 50 percent higher rates of mental disorders and substance abuse among persons self-identifying in surveys as lesbian, gay, or bisexual. Lesbian or bisexual women showed higher levels of substance abuse, while gay or bisexual men had higher rates of depression and panic disorder.
Sexuality and suicide
• Compared to heterosexuals, members of the non-heterosexual population are nearly 2.5 times the risk of suicide.
• Members of the transgender population are also at higher risk of a variety of mental health problems compared to members of the non-transgender population.
• The rate of lifetime suicide attempts across all ages of transgender individuals is estimated at 41 percent, compared to under 5 percent in the overall U.S. population.
• Compared to the general population, adults who have undergone sex-reassignment surgery continue to have a higher risk of experiencing poor mental health outcomes.
Sexuality and Intimate Partner Violence
• The weight of evidence indicates that the rate of intimate partner violence is significantly higher among same-sex couples.
Explanations for the Poor Health Outcomes: The Social Stress Model
• In attempting to account for the mental health disparities between heterosexuals and non-heterosexuals, researchers occasionally refer to a social or minority stress model.
• The social stress model probably accounts for some of the poor mental health outcomes experienced by sexual minorities, though the evidence supporting the model is limited, inconsistent and incomplete. However, this theory does not seem to offer a complete explanation for the disparities in the mental health outcomes.
• The social stress model deserves further research, but should not be assumed to offer a complete explanation of the causes of mental health disparities if clinicians and policymakers want to adequately address the mental health challenges faced by the LGBT community.
Gender Identity
• The concept of biological sex is well defined, based on the binary roles that males and females play in reproduction. By contrast, the concept of gender is not well defined. It is generally taken to refer to behaviors and psychological attributes that tend to be typical of a given sex.
• The scientific definition of biological sex is, for almost all human beings, clear, binary, and stable, reflecting an underlying biological reality that is not contradicted by exceptions to sex-typical behavior, and cannot be altered by surgery or social conditioning.
• The causes of cross-gender identification remain poorly understood. Research investigating whether these transgender individuals have certain physiological features or experiences in common with the opposite sex, such as brain structures or atypical prenatal hormone exposures, has so far been inconclusive.
• Studies show inconclusive evidence and mixed findings regarding the brains of transgender adults. Brain-activation patterns in these studies do not offer sufficient evidence for drawing sound conclusions about possible associations between brain activation and sexual identity or arousal.
• The current studies on associations between brain structure and transgender identity are small, methodologically limited, inconclusive, and sometimes contradictory.
• There is no evidence that gender identity is an innate, fixed property of human beings that is independent of biological sex (e.g., “a man trapped in a woman’s body”). The consensus of scientific evidence overwhelmingly supports the proposition that a physically and developmentally normal boy or girl is indeed what he or she appears to be at birth.
• Gender dysphoria — a sense of incongruence between one’s biological sex and one’s gender, accompanied by clinically significant distress or impairment — is sometimes treated in adults by hormones or surgery, but there is little scientific evidence that these therapeutic interventions have psychological benefits.
• Only about 0.6 percent of U.S. adults identify as a gender that does not correspond to their biological sex.
• Science has shown that gender identity issues in children usually do not persist into adolescence or adulthood, and there is little scientific evidence for the therapeutic value of puberty-delaying treatments.





